Artificial Heart Valves: Difference between revisions
No edit summary |
|||
| (2 intermediate revisions by the same user not shown) | |||
| Line 15: | Line 15: | ||
==Overview== | ==Overview== | ||
"The development of the heart valve design was fueled by the introduction of the heart-lung bypass machine,which was first used successfully on humans in 1953 to perform an atrial septal repair"[2]. More than 50 different heart valve designs have been developed since the first in 1952. Approximately three million heart valve replacements have occurred worldwide. "Currently over 290,000 heart valve procedures are performed annually worldwide and that number is estimated to triple to over 850,000 by 2050. Thus, the demand for artificial heart valves is expanding at a rate of 10-12% per year" [2]. | |||
===Heart Basics=== | ===Heart Basics=== | ||
The heart is one of two organs that make up the cardiovascular system; it pumps blood throughout the body. “The contractions of the heart necessary to drive the blood are controlled by electrochemical impulses created by pace maker cells” [2]. The pacemaker cells create the rhythmic contraction of muscle that is a person’s heartbeat. Heart valves are important to making the heart act as a pump. There are four heart valves: tricuspid, mitral, pulmonic, and aortic. These valves ensure that each muscle contraction produces efficient, unidirectional flow [2]. “On the right side of the heart, the tricuspid and pulmonic valves regulate the flow of blood that is returned from the body to the lungs for oxygenation, whereas on the left side, the mitral and aortic valves control the flow of oxygenated blood to the body” [2]. | The heart is one of two organs that make up the cardiovascular system; it pumps blood throughout the body. “The contractions of the heart necessary to drive the blood are controlled by electrochemical impulses created by pace maker cells” [2]. The pacemaker cells create the rhythmic contraction of muscle that is a person’s heartbeat. Heart valves are important to making the heart act as a pump. There are four heart valves: tricuspid, mitral, pulmonic, and aortic. These valves ensure that each muscle contraction produces efficient, unidirectional flow [2]. “On the right side of the heart, the tricuspid and pulmonic valves regulate the flow of blood that is returned from the body to the lungs for oxygenation, whereas on the left side, the mitral and aortic valves control the flow of oxygenated blood to the body” [2]. | ||
| Line 32: | Line 33: | ||
*Tricuspid Regurgitation | *Tricuspid Regurgitation | ||
*Tricuspid Valve Stenosis | *Tricuspid Valve Stenosis | ||
These issues can be caused by: congenital birth defects, ageing, and rheumatic fever among others. | |||
==Types of Artificial Heart Valves== | ==Types of Artificial Heart Valves== | ||
| Line 43: | Line 46: | ||
Mechanical valves are extremely durable and structural failures are nonexistent to very rare.[1] Major complications of mechanical valve replacement include thromboembolism, thrombosis, and lifelong anticoagulant therapy.[1] | Mechanical valves are extremely durable and structural failures are nonexistent to very rare.[1] Major complications of mechanical valve replacement include thromboembolism, thrombosis, and lifelong anticoagulant therapy.[1] | ||
The caged-ball valve has varied significantly over the years. The initial valve invented by Dr. Hufnagel "became obsolete with the introduction of the Starr-Edwardsd ball-and-cage valve in 1962" [2]. This design is as stated, a ball in a cage. | |||
===Tissue/Bioprosthetic=== | ===Tissue/Bioprosthetic=== | ||
| Line 65: | Line 70: | ||
==Transcatheter Heart Valves== | ==Transcatheter Heart Valves== | ||
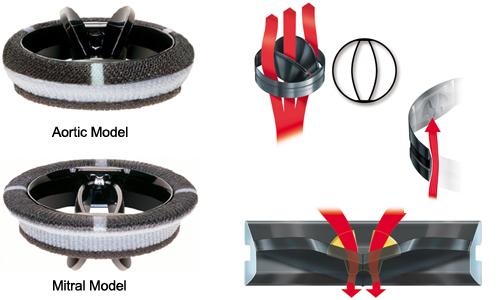
[[Image:transcatheter.jpg|left|thumb|150px|Transcatheter heart valve replacement in the closed position. [D]]] | [[Image:transcatheter.jpg|left|thumb|150px|Transcatheter heart valve replacement in the closed position. [D]]] | ||
Transcatheter heart valve replacement is the newest option in heart valve replacement. Rather than enduring open heart surgery a patient can have valve replacement via tiny incisions on thigh. The valves are expandable so they can travel up the vein. They are then pulled apart to fit and sewn in place. | |||
==References== | ==References== | ||
Latest revision as of 12:25, 28 February 2013
History

1952- First heart valve replacement using the caged-ball valve designed by a surgeon, Doctor Hufnagel. This valve did not replace the patient's diseased aortic valve but instead it was inserted in the descending aorta in an open-chest procedure.
1960- ball valves are introduced
1962- aortic homografts are introduced
1965- glutaraldehyde-preserved porcine 'bioprostheses'
1969- disc valves
1977- invention of bileaflet valves by St. John's Medical
Overview
"The development of the heart valve design was fueled by the introduction of the heart-lung bypass machine,which was first used successfully on humans in 1953 to perform an atrial septal repair"[2]. More than 50 different heart valve designs have been developed since the first in 1952. Approximately three million heart valve replacements have occurred worldwide. "Currently over 290,000 heart valve procedures are performed annually worldwide and that number is estimated to triple to over 850,000 by 2050. Thus, the demand for artificial heart valves is expanding at a rate of 10-12% per year" [2].
Heart Basics
The heart is one of two organs that make up the cardiovascular system; it pumps blood throughout the body. “The contractions of the heart necessary to drive the blood are controlled by electrochemical impulses created by pace maker cells” [2]. The pacemaker cells create the rhythmic contraction of muscle that is a person’s heartbeat. Heart valves are important to making the heart act as a pump. There are four heart valves: tricuspid, mitral, pulmonic, and aortic. These valves ensure that each muscle contraction produces efficient, unidirectional flow [2]. “On the right side of the heart, the tricuspid and pulmonic valves regulate the flow of blood that is returned from the body to the lungs for oxygenation, whereas on the left side, the mitral and aortic valves control the flow of oxygenated blood to the body” [2].
Reasons for Valve Replacement

- Mitral Valve Regurgitation (MR)
- Mitral Valve Prolapse and MR
- Mild to Moderate Left Ventricular Dysfunction and MR
- Atrial Fibrilation and MR
- Pulmonary Hypertension and MR
- Mitral Stenosis
- Mitral Valve Prolapse
- Aortic Stenosis
- Congenital Heart Valve Disease
- Pulmonary Valve Stenosis
- Tricuspid Regurgitation
- Tricuspid Valve Stenosis
These issues can be caused by: congenital birth defects, ageing, and rheumatic fever among others.
Types of Artificial Heart Valves
Mechanical

Mechanical Heart Valves were more common when heart valve replacement began.
- caged ball
- tilting disc
- hinged bileaflet
Mechanical valves are extremely durable and structural failures are nonexistent to very rare.[1] Major complications of mechanical valve replacement include thromboembolism, thrombosis, and lifelong anticoagulant therapy.[1]
The caged-ball valve has varied significantly over the years. The initial valve invented by Dr. Hufnagel "became obsolete with the introduction of the Starr-Edwardsd ball-and-cage valve in 1962" [2]. This design is as stated, a ball in a cage.
Tissue/Bioprosthetic

Complications
With any surgery there is always a chance of complications. “Problems common to all heart valve replacement devices include small but persistent risks of endocarditis and paravalvular leak.”[1] Thromboembolism is also a common complication in heart valve replacements due to atrial fibrillation; homographs are an exception to this rule. Mitral valve replacements have the highest risk of thromboembolism. Artificial heart valves (like any foreign implantation in the body) inflict what is known as a neodisease[1] that can cause side effects such as rejection. “If valve replacement is successful and uncomplicated, most patients experience an improvement in their symptomatic state, and therefore in their quality of life.” [1] Mortality post implantation is very rare; in most cases death is due to patient-related factors. [1] The following complications have directed future research into the design of artificial heart valves. Some main focuses of current and future research include: engineering living tissue heart valves and further study related to the fluid mechanics of the heart to enhance the direction of future mechanical heart valves. [2]
Specific to Mechanical

Structural failure is a risk associated with all mechanical devices; some types of mechanical valves have an increased risk. Mechanical heart valves require anti-coagulants to prevent build-up of plaque around the device. These anti-coagulants pose the potential for bleeding complications. “Hemolysis is more common with some types of mechanical valves, but is usually subclinical in the absence of valvular malfunction”[1] “These complications are believed to be associated with non-physiological blood flow patterns”[2]. “Mechanical heart valve designs have evolved significantly, with the most recent designs providing relatively superior haemodynamics with very low aerodynamic resistance. However, high shearing of blood cells and platelets still pose significant design challenges and patients must undergo life-long anticoagulantion therapy” [2].
Specific to Tissue
Leaflet tearing is an issue for all tissue-based heart valves regardless of donor. [2] “Bioprosthetic or tissue valves do not require anticoagulants due to their distinct similarity to the native valve geometry and haemodynamics, but many of these valves fail structurally within the first 10-15 years of implantation.”[2] “Tissue valve disruption is virtually inevitable, provided the patient lives long enough” [1].
Transcatheter Heart Valves
Transcatheter heart valve replacement is the newest option in heart valve replacement. Rather than enduring open heart surgery a patient can have valve replacement via tiny incisions on thigh. The valves are expandable so they can travel up the vein. They are then pulled apart to fit and sewn in place.
References
[1]Grunkemeir, Gary L. and Shahbudin H. Rahimtoola, “Artificial Heart Valves” Annual Review of Medicine 41 pp 251-63 (1990).
[2]Dasi, Lakshmi P. et al., “Fluid Mechanics of Artificial Heart Valves” Clinical and Experimental Pharmacology and Physiology 36 pp 225-237 (2009).
[3]http://www.nlm.nih.gov/medlineplus/ency/article/002954.htm
[C]http://www.aurorahealthcare.org/healthgate/images/diseased_aortic_valve.jpg
[A]http://circ.ahajournals.org/content/111/21/2850/F1.expansion.html
[B]http://circ.ahajournals.org/content/111/21/2850/F1.medium.gif
[D]http://triplehelixblog.com/wp-content/uploads/2012/02/heart-valve.jpg
[E]http://www.ctsnet.org/vendor_graphics/products/1038.jpg
[F]http://www.medtronic.com/mics/content/valve-mosaic-aortic-md.jpg
[G]http://cdn.medgadget.com/wp-content/uploads//2012/12/Colibri-Heart-Valve.jpg
[H]http://cdn.medgadget.com/wp-content/uploads//2012/12/crimped-valve.jpg
[I]http://www.reidhealthcare.com.au/images/product-onx-heart-valve.jpg
[J]http://www.clemson.edu/media-relations/archive/newsroom/multimedia/images/2008_images/september/pigvalve.jpg
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}